This page was reviewed under our medical and editorial policy by
Maurie Markman, MD, President, Medicine & Science
This page was updated on September 8, 2022.
Download prostate cancer infographic »
The prostate is a walnut-sized gland that’s part of the male reproductive system. Its key function is to produce a fluid that’s a component of semen.
Prostate cancer occurs when cells start growing out of control in the prostate. It’s an important health issue for all men to be aware of, because prostate cancer is the most common cancer in men after skin cancers, according to the National Cancer Institute.
The five-year survival rate for prostate cancer is 98 percent, according to the American Cancer Society (ACS).
Prostate cancer is typically treatable if caught early. More than 90 percent of prostate cancers are found when the disease is in the beginning stages, confined to the prostate and nearby organs.
Unlike screenings for breast cancer and colon cancer, there are no universal screening guidelines for prostate cancer. The U.S. Preventive Services Task Force (USPSTF) recommends that men age 55 to 69 weigh the benefits and risks before deciding whether they should undergo screening, which is typically performed with a blood test that measures levels of a protein called prostate-specific antigen (PSA).
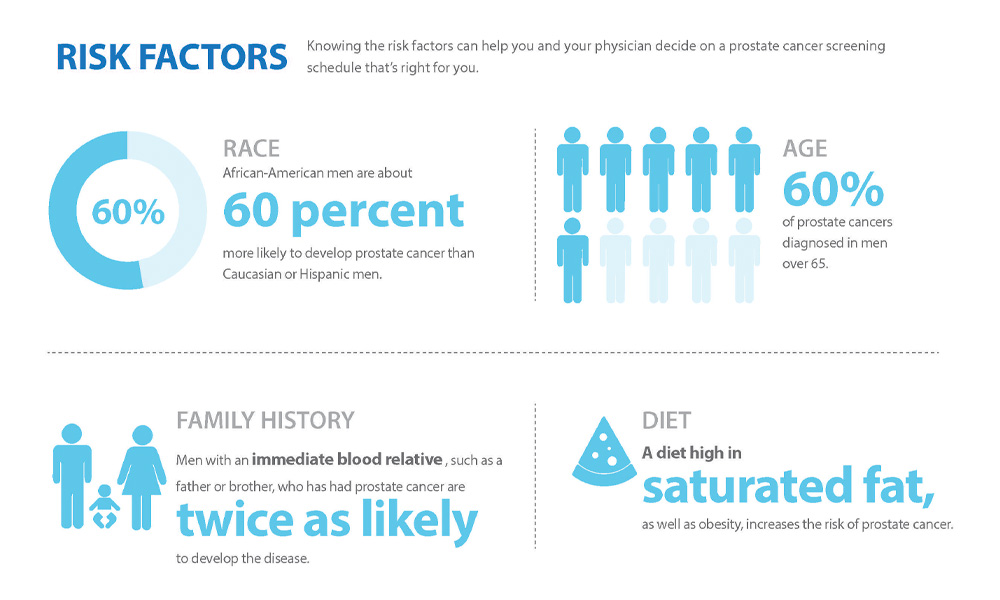
However, men in high-risk groups—such as those who are of African-American descent and/or have a first-degree relative diagnosed with prostate cancer before age 65—should consider speaking with their doctor about starting screenings at an earlier age.
Men older than 70 shouldn’t be routinely screened for prostate cancer, according to the USPSTF.
Regardless of age or risk factors, men should get checked if they suddenly experience issues with urination, erectile dysfunction or unexplained pain.
The USPSTF suggests that, before deciding on a screening, men should seek expert advice about the benefits and harms of screening. Risks may include:
The National Comprehensive Cancer Network suggests these screening guidelines and recommendations for men older than 45:
| Age | PSA level (ng/ml) |
DRE | Recommendation |
|---|---|---|---|
| 45-75 | Less than 1 | Normal | Get re-screened every two to four years |
| 45-75 | 1 to 3 | Normal | Get re-screened every one to two years |
| 75 or older | Less than 3 | Normal | Get re-screened every one to four years |
| 45 or older | More than 3 | Suspicious | Consider a biopsy or additional testing |
Prostate cancer is often detected during the course of a routine prostate exam and/or the PSA blood test, but diagnosing it may require other procedures.
PSA is a protein found in prostate cells that helps to keep semen liquified. Most cases of prostate cancer develop in these cells, so an elevated PSA count may be a sign of prostate cancer. However, PSA results are more of an indicator than a firm diagnostic tool—there’s not a certain PSA score that means a man has prostate cancer. Instead, there are various ranges that are considered average for different age groups. If the PSA score is elevated for your age, further testing may be recommended.
PSA levels are measured as ng/mL. According to the ACS:
Not all men with high PSA levels have prostate cancer. High levels may also be caused by a urinary tract infection, prostatitis or benign prostatic hyperplasia, all of which are noncancerous conditions. Conversely, men with a low PSA level may still develop prostate cancer.
PSA tests are not an indication of how aggressive the prostate cancer may be. Many prostate cancers are slow-growing and don’t require immediate treatment.
In addition to the PSA blood test, your doctor may perform a digital rectal examination (DRE). For this exam, your doctor inserts a gloved lubricated finger into the rectum to gently feel for any bumps or lumps on the prostate that could indicate cancer. The DRE isn’t typically painful and usually takes a few seconds.
Depending on the results of the PSA and DRE, the doctor may order a prostate biopsy. A biopsy may be performed through the wall of the rectum (known as a transrectal biopsy) or through the skin between the scrotum and anus (transperineal biopsy). Numerous tissue samples may be taken from different parts of the prostate. Samples are sent to a pathologist to examine under a microscope. This procedure allows the doctor to stage the disease and determine an appropriate treatment plan. After the procedure, patients may notice blood in the semen or after a bowel movement.
If a biopsy sample is found to contain cancer, the pathologist analyzing the specimen takes a deeper look at the cancer cells to determine how aggressive the disease is likely to be.
If the cancer cells appear significantly abnormal and dissimilar from healthy cells under a microscope, the cancer is considered more aggressive and expected to advance quickly. Conversely, cancer cells that look relatively similar to healthy cells indicate that it’s less aggressive and may not spread as fast.
Prostate cancers are assigned a Gleason score depending on how abnormal the cells look.
Gleason score: Gleason scores range from 2 to 10, going from least to most aggressive prostate cancers.
There are different types of cancer cells in a prostate tumor, so the final Gleason score is determined by adding the scores of the two main areas of the tumor.
First, the primary part of the tumor is assigned a number between 1 and 5. Lower numbers indicate that the cells appear relatively similar to healthy cells, while higher numbers show that the cells are abnormal-looking. Then, another number between 1 and 5 is assigned to describe the second most prevalent area of the tumor.
Finally, the two numbers assigned to the different parts of the prostate tumor are added. So, if most of the tumor is given a 4, and some of the tumor is more aggressive and given a 5, the final Gleason score would be 9.
Gleason scores of 6 or less are uncommon, and these prostate cancers are considered low-grade or not aggressive. A Gleason score of 7 is given to intermediate-grade cancers. A Gleason score of 8 to 10 is considered high-grade or aggressive.
Biomarker testing: In some cases, a biomarker test is recommended to certain people with prostate cancer. These tests are most often suggested if you have low- or intermediate-risk prostate cancer and are a candidate for active surveillance. This approach involves delaying treatment until there are signs that the cancer is worsening. These patients may benefit from biomarker tests, as these help inform whether the cancer is likely to grow and spread quickly or slowly.
Knowing this information helps doctors figure out the best way to manage and treat cancer. For example, if your doctor is considering delaying treatment and monitoring your condition with active surveillance and then a biomarker test reveals that the cancer is fast-growing, the plan may change. You and your doctor may reconsider the plan and initiate treatment sooner.
Biomarker tests may be performed on a sample of blood or other bodily fluids, but usually the tissue removed during a biopsy is used. If prostate cancer is discovered after a biopsy, for example, biomarker tests may be performed on the same sample to analyze the genetics of the cancer cells within the specimen.
There are many biomarker tests, including:
If you’re considered a candidate for biomarker testing, your doctor may discuss this option with you, including the potential advantages and drawbacks.
After a biopsy, the patient’s tissue sample is sent to a laboratory, where a specialized doctor called a pathologist studies it under a microscope.
The pathologist is looking to see whether the cells are cancerous. After the pathologist comes to a conclusion, the results are returned to your doctor. Biopsy results are usually delivered within days of the procedure.
Typically, the results reveal one of three findings.
A suspicious result indicates that the biopsy sample contained some abnormalities but no cancer was found. There are a couple of potential explanations for a suspicious prostate biopsy result, including:
Prostate biopsies sometimes return false-negative results. Although numerous samples are taken from the prostate during a biopsy, the needles may fail to collect cells from an area of the prostate that contains cancer, resulting in a false-negative result.
Your care team is aware that false-negatives occur and may consider a negative biopsy result in the context of other tests. For example, if you have an elevated PSA level but a negative biopsy result, your doctor may recommend that a biomarker test be performed on samples of blood, urine or the existing biopsy specimen to take a deeper look at the cells. In some cases, your doctor may even suggest a second prostate biopsy.
Below are imaging tests that may be used to determine the type, stage and progression of a patient’s prostate cancer.
Bone scan: Prostate cancer may metastasize to the bones. If a patient is experiencing bone pain, or blood tests reveal elevated calcium levels, an oncologist may perform a bone scan to determine whether the prostate cancer has spread to the bones. During a bone scan, a doctor injects a small amount of low-level radioactive material that shows up in affected regions of bone when images are taken, pinpointing where the cancer is located.
Computed tomography (CT) scan: A CT scan reveals blood flow and anatomy of tissues in and around the prostate, allowing for a diagnosis and the monitoring of tumor growth. This type of scan is generally used for prostate cancer if other test results suggest that the cancer has spread outside of the prostate. It is most useful for detecting prostate cancer that has metastasized to nearby organs or lymph nodes.
Magnetic resonance imaging (MRI): An MRI may be especially useful for the prostate, due to greater soft tissue contrast. MRIs may help determine whether a biopsy is needed, improve the accuracy of biopsies, and detect cancer spread. This type of scan renders a clearer picture of the inside of the prostate gland than a CT scan and can more accurately detect and reveal cancer within the prostate.
Positron emission tomography/computed tomography (PET/CT) scan: A PET (positron emission tomography)/CT scan is an advanced nuclear imaging technique that combines CT scan technology with positron emission tomography in one machine. A PET/CT scan shows both the structure and function of cells and tissues in the body during a single imaging session. In the case of prostate cancer, this scan provides a more comprehensive view of the pelvis to determine the presence of abnormal activity, even before a tumor may have developed. When other tests suggest that prostate cancer has metastasized, a PET scan can help uncover where it has spread in the body. However, the images produced by a PET scan are less precise than those of an MRI or CT scan. A PET-CT scan combines the strengths of the PET scan in exposing potentially cancerous areas throughout the body, while also providing more clarity and detail through the CT images.
Transrectal ultrasound (TRUS): During this imaging test, a small probe is inserted into the rectum. It gives off sound waves that are used to create an image of the prostate. TRUS may help doctors make a diagnosis, know where to position tools during a biopsy, and guide brachytherapy treatment, which is a type of internal radiation therapy used to treat prostate cancer.
The most common lab test for prostate cancer is advanced genomic testing, which examines a tumor to look for DNA alterations that may be driving the growth of the cancer. By identifying the mutations that occur in a cancer cell’s genome, doctors may get a clearer picture of the tumor’s behavior and be able to tailor a patient’s treatment based on the findings.